Read this before buying Christian Jarrett’s Great Myth of the Brain
Jarrett creates his own Great Brain Myth
Plus: ‘10% of our brains’ answer that eluded mythbuster Jarrett
The first thing a curious person does when they hear about Neurofeedback for the first time is Google it, and on page 1 up comes an article by Christian Jarrett from February 2013 titled ‘Read this before paying $100s for neurofeedback therapy’.
This article is often cited as undermining Neurofeedback by the casual reader, and it seems that was the author’s intent, but if you dig into the substance of the article and the comments, this is far from the case.
The inquisitive and intelligent reader prepared to scratch the surface of Jarrett’s writing will find that the article highlights several misunderstandings and misrepresentations of Neurofeedback, rather than undermining it.
Jarrett has built a career as an expert in debunking ‘myths’ of the brain. He even wrote a book ‘Great Myths of the Brain’, inspired by a previous book ‘Mind Myths’.
Jarrett’s book ‘borrows’ heavily from the earlier one, specifically from chapters by professional sceptic Barry L Beyerstein. They both wrote chapters on the myth we only use 10% of our brains, and admitted they didn’t know the answer.
If you care to read this article to the end, I will answer the question that both Jarrett and Beyerstein failed to answer, which is where the 10% myth actually came from.
In the article, Jarrett makes 7 key points.
Some of these points are valid, but the others demonstrate the reasons Atul Gawande identifies as ‘Why Doctors Fail ?’: Ignorance, Ineptitude and Hubris.
Of course, this Dr Christian isn’t a medical doctor, but we believe that these criteria are just as valid when assessing a scientific critic’s ‘fitness to practice’.
So what exactly does Dr. Christian Jarrett say ?
- Neurofeedback practitioners ‘can’t make up their minds whether to clothe themselves in the white coats of science, or to dress up in the loose robes of woo’.
- The Sunday Times printed a ‘sensationalist’ article about a Neurofeedback practice called BrainWorks in London.
- The marketing language used by BrainWorks isn’t to Jarrett’s taste, tending to ‘big up their technical wizardry’.
- The idea that using neurofeedback to induce alpha brainwaves could induce states of mind associated with alpha brainwaves was ‘debunked’ by a professional sceptic called Barry Beyerstein years ago.
- The more recent studies on the inducement of alpha waves to improve mood use a variety of protocols and in Jarrett’s opinion ‘tend to be of poor quality, lacking control groups and proper blinding’.
- Neurofeedback is used increasingly to treat psychiatric and developmental issues, and the evidence base is growing.
- Neurofeedback practitioners ‘make grandioise claims, like the changes being permanent’.
We have observations (as do the other 230+ commenters) about all these points, but it is the first one that completely misses the point and shows why Christian’s assumed authority to speak on such matters should itself be regarded with scepticism …
Christian Jarrett’s Great Myth of the Brain
The criticism at the heart of the article is ‘Neurofeedback practitioners ‘can’t make up their minds whether to clothe themselves in the white coats of science, or to dress up in the loose robes of woo’.
This is his myth: Neurofeedback cannot be both a therapeutic technique to improve mental health, and a tool to enhance spiritual development or consciousness.
The author assumes that mental health and spiritual development are so very different that the same tool could not possibly be relevant to both, and that practitioners that suggest they can help in both areas undermine their very credibility by mixing the two.
This assumption is fundamentally flawed and shows ignorance of the fields of mental health and spiritual development. Any psychologist worth his salt is aware of the growing evidence of the effectiveness of ‘mindfulness’ practice to address mental health issues.
‘Mindfulness’ is essentially Buddhist practice without the Buddhist label and cultivating ‘mindfulness’ is at the heart of spiritual development, which ultimately is about expanding your awareness so that you have more choices; the more choices we have the more resourceful we are and the better we are able to cope with the challenges of life.
As we become more mindful we can create distance between ourselves and our thoughts so we are no longer owned by our thoughts, instead we have thoughts, we can choose how we react to them.
So it is no wonder that mindfulness practice can assist with many forms of mental health wellbeing – from the lack of impulse control in ADHD children, to the hyper-vigilance of trauma victims, to the ruminating negative thoughts of depression.
What good mental health and mindfulness practice have in common are the ability to shift between ‘brain gears’ as appropriate.
So what does this mean for the practice of a tool such as Neurofeedback that to improve brain regulation ? It means that the mechanism is essentially the same, whether we are dealing with a severely traumatised and depressed brain or an Olympic athlete’s brain – we are improving brain regulation or the ability to shift ‘brain gears’ smoothly when required.
And using the same tool for both mental health improvement and spiritual development is not ‘worrying’ or ‘far reached’ – to someone who understands the subjects it makes absolute sense.
We address the other six points one by one below:
Point 2. The Sunday Times printed a ‘sensationalist’ article about a Neurofeedback practice called BrainWorks in London.
The article was a glossy Sunday paper supplement, not a scientific journal, and was written to inform and entertain. Yes, the journalists may have glossed over a few points, and BrainWorks won’t have had editorial control so could not correct any factual errors.
So we agree it could be described as ‘sensationalist’, but not unexpectedly so in its context.
Point 3. BrainWorks’ marketing language ‘bigs up their technical wizardry’.
We understand and sympathise with this point; every business will adopt marketing language that reflects its culture and values.
At BrainTrainUT we have sought to earn a reputation as ‘the Neurofeedback practice you can trust’ by being straight forward with our marketing language and avoiding hyperbole.
Point 4. The idea that using neurofeedback to induce alpha brainwaves could induce states of mind associated with alpha brainwaves was ‘debunked’ by a professional ‘skeptic’ called Barry Beyerstein years ago.
Beyerstein was the founder and Chair of the ‘Britsh Columbia Skeptics Society’.
He also wrote two chapters in the 1999 book ‘Mind Myths’, the inspiration for Jarrett’s 2015 book ‘Great Myths of the Brain’, both published by Wiley.
The first Chapter was titled ‘Whence Commeth the Myth that We Only Use 10% of our Brains’. If you are truly interested in the answer don’t bother reading the book as you won’t find out. Beyerstein never answered the question. This ignorance, ‘despite years of digging’, didn’t stop him going off at multiple tangents to invent his own myths, blaming numerology and the ‘self-improvement industry’ for disseminating the belief.
In Jarrett’s book he couldn’t resist including a Chapter titled ‘We Only Use Ten Percent of Our Brains’, which added no more to our understanding of the source of the myth than Beyerstein had offered 16 years before.
Beyerstein’s inability to answer his own question didn’t stop him from writing at length about ‘brain tuners’, beginning with his belief that ‘many citizens of the industrialized world still approach electricity as if it were some kind of magical force’ (this was 1999).
If you cut through the waffle, Beyerstein says the following about alpha neurofeedback:
- There was a ‘bandwagon’ of alpha neurofeedback devices that used ‘cheap circuitry’.
- They were based on the unproven assumption that conditioning your EEG to generate the alpha waves seen in long-term meditators equated to entering a meditative state.
- Advocates confused correlation with causation.
The problem with his argument is that some intervention effects are by nature subjective (internally experienced), not objective (externally measurable). A state of enlightenment is one of these. It’s always going to be able to difficult to ‘prove’ such an internal experience through scientific measurement.
Point 5. The more recent studies on the inducement of alpha waves to improve mood use a variety of protocols and in Jarrett’s opinion ‘tend to be of poor quality, lacking control groups and proper blinding’.
A common theme in Jarrett’s writing is that anything less than double-blinded placebo-controlled studies is ‘poor quality’ evidence. In making this judgement he condemns the estimated 70% of medical interventions that have not been evidenced to this standard.
He ignores the fact some interventions are simply not suited to this sort of experiment.
With medications it is easy to create placebo versions of pills that look exactly the same so those prescribing the drugs and the patients receiving them don’t know whether they have received the real drug or the placebo version, the so-called ‘double-blinded placebo’.
Any intervention more complex than taking a tablet is more complex to create a placebo – you have to create a ‘sham’ treatment that is experienced as the real thing by both the practitioner delivering and the patient/client receiving the intervention.
This can be practically impossible – imagine trying to conduct a ‘sham’ session of talking therapy where the therapist talks nonsense but this doesn’t come across as nonsense to the patient.
It can be ethically problematic – imagine trying to recruit a group of 100 school children to an experiment involving a 2 hour round trip, twice a week for 3 months, in the knowledge that it might be ‘fake’ neurofeedback.
And it can be technically challenging and costly – imagine having to design complex equipment and software that works at multiple levels – at one level the practitioner thinks they are conducting a real intervention, yet at an another level the equipment is being controlled so that it ‘looks like’ a real intervention even though it is in fact a sham.
These arguments also ignore the fact that the first clinical application of neurofeedback was discovered completely by accident, in possibly the ultimate ‘double-blinded’ study when a UCLA sleep researcher Dr Barry Sterman discovered that neurofeedback could reduce seizures in cats.
The standard of evidence demanded by independent assessment authorities are randomised controlled trials (RCTs), where the experimental group (doing Neurofeedback) is compared to a control group(s), which does another intervention, or nothing. And there are many such studies.
Jarrett refers to multiple studies comparing different protocols of Alpha wave neurofeedback as if that is a weakness in the field.
In 1974 Barbara Brown collated 574 studies on Alpha waves she called ‘The Alpha Syllabus’, and research continues 40 years on.
Multiple protocols are not necessarily a weakness.
For example in our own practice at BrainTrainUT we can use alpha in at least 5 ways:
1. To enhance alpha amplitude;
2. To enhance alpha synchrony between hemispheres;
3. To enhace alpha sychnrony between the front and back of the head;
4. To use alpha and theta rewards together to induce a deep-state known as Alpha-Theta to address deep trauma and addiction, or enhance creativity; and
5. To enhance alpha synchrony between couples.
Some of these protocols are more experimental than others, which is the nature of the field; responsible practitioners will explain the differences, and those who wish to progress the field will continue to experiment. We contend this is a strength, not a weakness.
Point 6. Neurofeedback is used increasingly to treat psychiatric and developmental issues, and the evidence base is growing.
We agree, and when the body of evidence has been reviewed by independent bodies such as PractiseWise, who conduct research on psychosocial interventions for organisations such as the American Academy of Pediatrics, they reach the conclusion that the evidence reaches the highest standards in the field.
The evidence base for Neurofeedback for clinical conditions continues to grow, and the ISNR database at the time of writing includes 705 published studies.
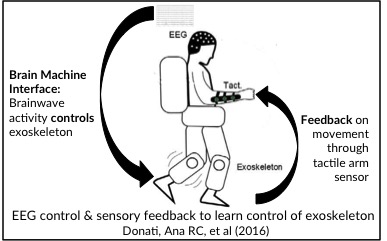
The ability of the brain to learn to make sense of information (habitual learning) is not questioned by science. Recent examples of research and practical application include:
- Paraplegic patients learning to control the bionic legs of exoskeletons using their EEG for the control output and tactile feedback for sensory input:
- The ability of mechanical robots with biological brains with a distance sensing input to learn to steer away from walls:
- Implants to create new neural channels that the brain learns to decode and/or control:
- Cochelar ear transplants take in auditory information and transmit electrical signals via the auditory nerves; after a while the brain decodes this as audio.
- Kevin Warwick used an implant in his nervous system to control a robotic arm using a 2-way link across the Atlantic, and to communicate with his wife with a similar implant.
Point 7. Neurofeedback practitioners ‘make grandioise claims, like the changes being permanent’.
There is solid evidence for the permanence of changes both functionally and physically. Two studies below demonstrate physical changes.
This 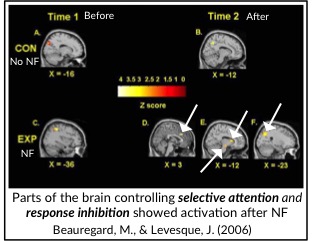 study used fMRI imaging to show changes in brain activation after Neurofeedback.
study used fMRI imaging to show changes in brain activation after Neurofeedback.
These changes were in the areas of the brain associated with selected attention and response inhibition.
This was consistent with reported changes in behaviour.
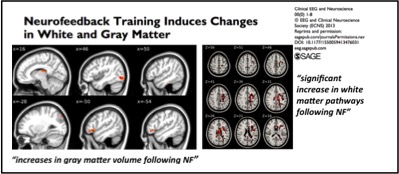
This study showed increases in gray and white matter following Neurofeedback:
There should be little doubt the changes are real and permanent, just as in the examples against Point 6 above.
The answer to the 10% question
We can reveal the truth that eluded the great myth busters Jarrett and Beyerstein despite years of effort. The answer is it was the work of Pierre Flourens, a critique of the work of Franz Joseph Gall, who founded phrenology, the once fashionable idea that your personality was reflected by the lumps and bumps on your skull.
Although Flourens was driven by religious reasons, he could be described as the first neuroscientist, and in the 1820s he conducted experiments to remove parts of the brain and determine what effect they had.
It was when experimenting on birds and rabbits he found that he had to remove up to 90% of the cortex before functions like wing flapping and eating were affected.
In reality these are sub-cortical functions, so the conclusion was flawed, but the myth was born.
Thanks to David Kaiser for this last nugget, and thanks for reading.
Stuart Black
October 2017.
P.S. Addition of studies post-script
Jarrett has added further studies as post scripts to his original post that appear to be a disingenuous attempt to undermine the field despite his assertions that he does not have “some mysterious vendetta” against neurofeedback.
Above we described the challenges involved in the creation of double-blinded sham-controlled trials for neurofeedback, the ethical issues involved in getting studies approved, and the fact that neurofeedback was discovered for neurological conditions though possibly the ultimate fully-blinded experiment.
Despite this, there are a group of researchers who have conducted trials of attempts to conduct sham-controlled neurofeedback trials.
It is these experiments, and only these experiments, that Jarrett has added to his blog. That seems disingenuous.


